
Higher mortality rates in Hindus vs superior survival rates of Muslims: A data analysis

What is certain is that obsessing about the Muslim population in India will not decrease the high Hindu mortality rates. While putting a dedicated effort and a political will towards achieving a healthier diet and social practices may bridge the survival differentials.
By Amna Meraj, TwoCircles.net
Right after the Gujarat riots in 2002, the then Chief Minister of Gujarat Narendra Modi remarked on the Muslim pogrom survivors in a refugee camp by the words, “Hum paanch humare pachees”. The Rashtriya Swayamsevak Sangh (RSS), which is a right-wing, Hindu nationalist, paramilitary volunteer organization promotes Hindu Rashtra and views the increase in Muslim population as a ticking bomb. Gone are the times when it merely propagated that birth control is not practised by Muslims, a kid-glove approach in front of what the outfit’s ideologues in recent times have started propagating. From “Four wives and forty children,” it progressed to grave allegations against the entire Muslim community of a deliberate “population jihad” or if you are a reader of Yugaparivartan, a “demographic siege of Al-Hind”.
Propaganda certainly achieves short term objectives and political motives but if history is to be believed, does long term damage.
Let us try to decipher fantasy from reality to avoid such damages which are rampant in society.
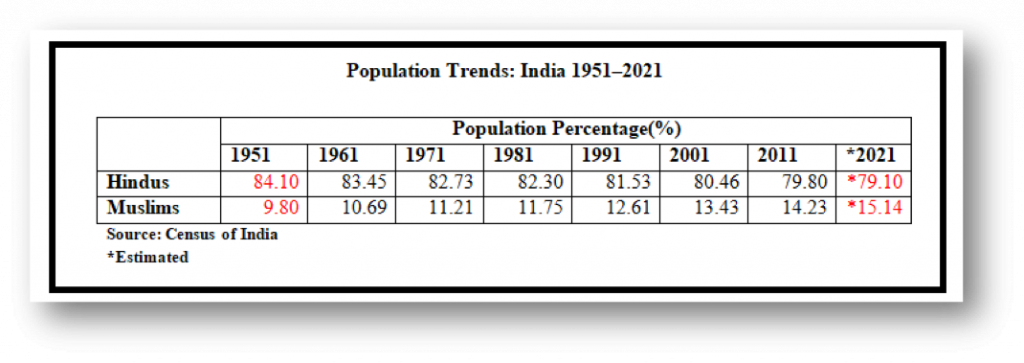 Table1: Population trends in India from 1951 t0 2021.
Table1: Population trends in India from 1951 t0 2021.
It is true that Hindu population of India has seen a persistent decline in its percentage proportion since independence. However, the central question is this: Is this a result of an attempt at ‘population jihad’, or perhaps a puzzling high Hindu mortality rate and better Muslim survival rate?
The discourse often ruminates around the high fertility of Muslims or on the hope that better socio-economic conditions would decrease fertility. In demography, apart from fertility and migration, mortality has a significant impact. Higher fertility amongst Muslims has appreciable social consciousness in India and interestingly, higher mortality amongst Hindus is sadly unnoticed.
Mortality Rates
The Muslim-Hindu survival differential has been evident since the past seven decades.
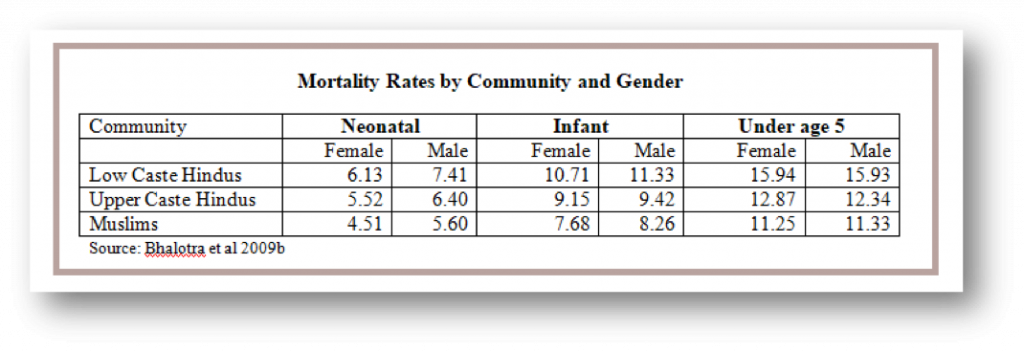 Table2: Minority rates by community and gender.
Table2: Minority rates by community and gender.
By age five, the Muslim advantage over Hindus is about 17% of baseline mortality risk. The persistent and large child survival advantage exhibited by Muslims is remarkable only because it is despite their socioeconomic disadvantage. Perplexingly, the upper caste Hindus who enjoy a significant advantage in their socio-economic status (SES) have higher mortality than Muslims whose survival rates are higher and undeterred despite their disadvantaged SES. Clearly, SES is not the main player here.
Child Sex Ratio
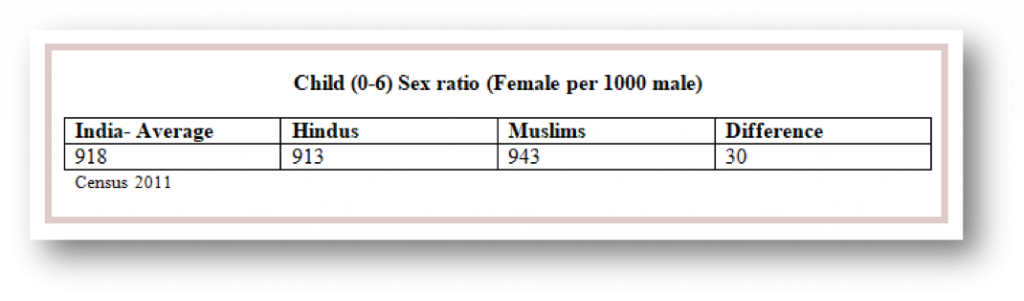 Table3: Child Sex Ratio
Table3: Child Sex Ratio
Around 5,00,000 girls are being ‘lost’ (euphemism) annually through female feticide in India.
A part of the reason for mortality amongst Hindus is actually driven by excess mortality amongst females. Hindu girls face higher under-5 mortality risk than infant mortality risk; consistent with the view that for female at a higher age, the role of parental preferences of gender becomes more relevant than the role of natural survival. Hindus may be less careful about their daughter’s health than Muslims because of higher male preference in Hindus, e.g., due to the extreme role of dowry (groom received), and the importance Hindus attach to having sons perform religious rites.
The sharpest sign of gender preference is the extent of female feticide by religion. Research shows how sex-selective abortion started earlier and remains more prevalent amongst Hindus. Muslims exhibit higher gender equity with a lower sex ratio at birth and a smaller gender gap in child mortality. This demonstrates better survival chances amongst girls as a prime explanation of the overall Muslim advantage.
Maternal Health and Diet
Muslim boy survival is also higher than Hindu boys and cannot be explained by gender preference. Most of the survival advantage of Muslims over upper caste Hindus is apparent soon after birth making better Muslim maternal health a crucial factor. Higher gender equity ensures better maternal health in communities. Across three decades, Indian Muslim women gained height (a function of childhood nutrition) more rapidly than Muslim men, while Hindu women lagged behind their men (and behind Muslim women). A mother’s height lowers child mortality and this makes a significant contribution to the religion gap. Indian Muslims largely originated in the northern Indian subcontinent, with a racial stock typically taller and bigger build which may further contribute to the height gap.
Height is an indicator of cumulative nutrition over the life-course, whereas Body Mass Index (BMI) is for short term health. Muslim women also have healthier BMI. Hindu women were often undernourished than Muslim women (37% against 32%). Muslim mothers eat meat, eggs and even dairy products way more than Hindu mothers. Children with vegetarian mothers are shown to have higher mortality. It is only at higher living standards that Vegetarianism probably does not adversely affect health. Amongst the poor, a vegetarian diet may not provide sufficient nutrition.
Better child nutritional status also matters. For example, Wasting Syndrome (lower than normal body mass and fat tissues) is seen less frequently in Muslim kids than their Hindu counterparts. It may be directly linked with intake of sufficient protein. A mortality advantage has been observed for Muslim adults as well as children suggesting that religious differences in diet (complete avoidance of meat by some Hindu sects) may matter over the life course.
Muslim Survival Advantage
Muslims have poorer SES, higher fertility, shorter birth-spacing, and are a minority group in India that may live in areas with relatively poor public provisions; despite all these factors that increase mortality rates, Muslims have actually persistently achieved substantially higher child survival rates than both low and high caste Hindus. If child mortality rates amongst Hindus were to converge to the level exhibited by Muslims, Hindus would avert 0.37 million under-5 deaths each year.
By age five, the Muslim survival advantage over upper-caste Hindus, who enjoy unambiguously higher SES than Muslims, is about 10% of baseline mortality risk. This means 1,27,955 excess under-5 deaths amongst high-caste Hindus and 2,44,535 among low-caste Hindus annually.
There remains some ‘unexplained’ Muslim survival advantage. Differences in observed heights and weights of children between communities are small yet differences in survival rates are large. Bhalotra (University of Bristol) writes “these findings motivate the investigation of attitudes and unobserved behaviours Muslims might have, unlocking the key to a significant impact on average mortality rates in India.”
Overall, the evidence points to a persistent Muslim Survival “fixed effect”, puzzling demographers world over.
Researchers concluded that there is something peculiar to health that Muslims are “good at” and showed that Muslims have stronger health and social capital.
Religious rules regarding healthier behaviour that may matter are: the hygiene and specially hand hygiene resulted by multiple ablutions for daily prayers, the higher percentage of toilet usage and washing of private parts after urination as well as passing stool, for infants and adults.
Another relevant religious rule is the avoidance of all intoxicants and thus alcohol in the Muslim community. Data indicates a significantly larger share of Hindu respondents drink alcohol compared to Muslims.
Several partial reasons for the observed Muslim survival advantage over Hindus:
- Relatively more meat-based diet.
- Closer kinship i.e. stronger social capital.
- Relatively earlier initialization of breastfeeding.
- Less differential treatment for children by birth-order.
- Lower degree of son-preference and thus resulted in a higher degree of gender equity.
- Taller and less likely to be undernourished mothers and their lower propensity to work outside the home.
- Awareness of the importance of fluids in treating diarrhoea in children, greater likelihood of taking a child with diarrhoea to a facility for treatment.
Child mortality
Non-disposal of faeces spreads disease-causing pathogens and open defecation is substantially (40%) higher in Hindus than Muslims. Michael Geruso (University of Texas) reveals how this major sanitation difference explains the differential child mortality patterns revealing a Muslim neighbourhood survival advantage as it decreases open defecation percentage.
Adult Mortality
Religious differences in adult mortality are consistent with the patterns of infant and child mortality. The research “Role of Religion in Fertility Decline: The Case of Indian Muslims” found mortality higher for Hindus at every age. This research, though not recent, is one of the most comprehensive researches done on this topic. The Muslim crude death rate on average was found to be lower than that of Hindu’s by 13%.
The Median age of Muslims is younger than the median age of Hindus. That means the average Muslim population is younger than the average population of Hindus. Muslims indeed have more reproductive and working years ahead of them and have higher fertility than Hindus. However, this neither explains nor influences the high Hindu mortality. These are two distinct factors. What is certain is that obsessing about the Muslim population will not decrease the high Hindu mortality rates. While putting a dedicated effort and a political will towards achieving a healthier diet and social practices may bridge the survival differentials.
Amna Meraj has done post-graduation in Anthropology from Pune University (SPPU), India.